
Thursday, June 25, 2020
Inside the U.S.’s Largest Maximum-Security Prison, COVID-19 Raged. Outside, Officials Called Their Fight a Success.

Terry Rogers holds a photo of Michael Williams, her brother, in front of her home in Bridge City, Louisiana, on May 17, 2020. (Kathleen Flynn/ProPublica)
By the time he persuaded the guards to let him call his family, Michael Williams could feel his life slipping away. His body ached, and he was struggling to breathe. For three days, he had been locked behind the heavy metal door of a cramped prison cell, terrified and alone.
“They weren’t treating him,” his son, Kevin Cooks, recalled. “He kept telling me, ‘Son, I’m going to die in here.’” Williams, a 70-year-old diabetic, was serving a life sentence for a 1974 convenience store murder he had always maintained he did not commit. It was the first time his son had ever heard him cry.
Williams’ family and his lawyer called over and over to the Louisiana State Penitentiary in Angola, pleading with guards and nurses to have him moved to a hospital. When they finally reached one of the senior guard officers, family members said, he told them Williams didn’t have the virus.
On May 7, a nurse assured one of Williams’ sisters that he was improving. The next day, he was rushed to a regional hospital in critical condition. The day after that, a doctor called to say Williams had gone into cardiac arrest. If they wanted to say goodbye, he said, they should hurry.
While the novel coronavirus burned through Angola, as the country’s largest maximum-security prison is known, officials insisted they were testing all inmates who showed symptoms, isolating those who got sick and transferring more serious cases to the hospital in Baton Rouge, about 60 miles to the south.
But from inside Angola’s walls, inmates painted a very different picture — one of widespread illness, dysfunctional care and sometimes inexplicable neglect. They said at least four of the 12 prisoners who have died in the pandemic, including Williams, had been denied needed medical help for days because their symptoms were not considered sufficiently serious.

Janet Clark, left, embraces her sisters Rogers, middle, and Noel Fluence, right, after the funeral service for Williams, their brother, on May 18, 2020. Williams contracted COVID-19 while incarcerated at the Louisiana State Penitentiary at Angola. (Kathleen Flynn/ProPublica)
“If you do that testing, how are you going to handle the results?” the former official, Dr. Raman Singh, asked. “If you find it is widespread, how do you handle that with your guards? Never ask a question if you aren’t going to like the answer.”
A spokesman for the corrections department, Ken Pastorick, would not disclose the number of inmates who have been tested at Angola. Nor would he comment on allegations that the authorities had deliberately withheld tests from many prisoners who showed symptoms of the virus.
“We are proud of the job we have done managing the pandemic thus far,” he said, “and the results bear out that our plan continues to be successful.”
Yet, in the two months after Louisiana prisons recorded their first cases of the novel coronavirus in late March, the corrections department tested only about 3% of the roughly 14,150 men incarcerated in state prisons, official figures indicate. The authorities have since conducted about 400 more tests.
Prisons and jails now account for most of the biggest COVID-19 hot spots in the country, with thousands of cases documented at penitentiaries in Texas, Ohio, California and other states. But corrections officials have reported striking differences in the impact of the virus.
As some states have begun mass testing, they have found prison infection rates as high as 70%. Yet, a surprisingly low death rate in prisons across the country has allowed some officials to downplay or even hide the spread of the virus behind bars.
Even prisons like Angola, with older male inmates who are particularly vulnerable to the disease, have not shown mortality rates close to those of nursing homes. A recent New York Times analysis showed that nursing homes accounted for about 11% of the country’s coronavirus cases but 35% of deaths.
A ProPublica investigation of the coronavirus outbreak at Angola — long the most troubled prison in a state with the country’s highest inmate mortality rate — offers a vivid, inside look at how some dramatic and largely unseen chapters of the COVID-19 crisis have unfolded.
This article is based on telephone conversations, email messages and other communications with more than two dozen Angola inmates, as well as interviews with many lawyers and relatives who have been in touch with them and a review of more than 900 email reports sent by inmates to a prisoner support group during the pandemic. It also draws on interviews with current and former officials, and statements and documents produced in two federal lawsuits over medical treatment at Angola.
In many cases, prisoners said, inmates who were obviously sick with the coronavirus were denied even cursory medical examinations, mostly because they did not register sufficiently high fevers. Men passed out and were told they were dehydrated. Others, who complained of bad coughs, aches, fatigue and stomach pains were treated with Tylenol, Pepto-Bismol and Tums.
Countless sick prisoners were left to recover in their bunks, which are typically set less than 4 feet apart in Angola’s crowded dormitories. Firsthand accounts from 11 of those dormitories, which collectively house nearly 1,000 inmates, suggest that most of the men inside became infected.
Some sick prisoners concealed their symptoms to try to avoid losing their freedom of movement and other privileges to extended quarantines, inmates said. But the efforts at containment have also been haphazard, they added, with sick prisoners frequently brought back to quarantined areas and staff moving between dorms that were under quarantine and others that were not.
Perhaps the most serious problem has been Angola’s unwillingness to test inmates more widely.
Like other parts of the country, Louisiana did face testing shortages early on. However, the corrections department’s former medical director, Dr. John Morrison, said there were thousands of test kits available to the prisons when he left that job in mid-April. Official reports show that the corrections department also obtained 4,100 more tests a month later.
Yet, even after public health officials began to urge widespread testing in prisons and Gov. John Bel Edwards promised such screening, Angola has moved very slowly to increase testing, official statistics show. According to national statistics compiled by the COVID Prison Project, a nonprofit public health group, Louisiana’s reported testing rate trails far behind other states that have suffered serious outbreaks.
Louisiana corrections officials have not reported any testing or infection figures for the 13,844 state prisoners who are held in more than 100 parish jails under a long-standing arrangement to relieve overcrowding.

Haller Jackson prepares to leave Angola after completing his five-year sentence this month. (Kathleen Flynn/ProPublica)
Louisiana is hardly the only state that has been slow to test prisoners. Only Michigan and Tennessee had tested more than half of their inmates by mid-May. Since then, however, at least nine others have done so.
The accounts from Angola inmates and others cast new light on the prison’s health care system, one that has been a focus of criticism, litigation and halting reform for almost half a century.
Lawyers for a dozen inmates who filed a class-action lawsuit in 2015 argued that Angola’s medical care was so egregiously poor, it violated the Eighth Amendment’s prohibition against cruel and unusual punishment. The federal judge hearing the case in Baton Rouge, Shelly D. Dick, said in February that she will find the state’s practices “unconstitutional in some respects,” but her final ruling is still pending.
Nearly all of the doctors who work full time at Angola ended up there after the state medical board suspended their licenses for violations ranging from drug dealing to sexual misconduct. The prison’s medical director, Dr. Randy Lavespere, served a federal prison sentence for buying $8,000 worth of methamphetamine in a Home Depot parking lot. He is now overseeing health care for the entire corrections department.
Inmates describe some of the doctors, nurses and paramedics as able and well-intentioned. But they and their advocates said the staff was unable to deal adequately with the day-to-day medical problems of its 5,500 inmates long before the virus hit.
Cancers and other slow-growing diseases are often discovered late — sometimes after years of medical complaints that were ignored. Prisoners with chronic illnesses have often had trouble getting specialized care or even regular medication. Louisiana prisons have long punished inmates who are determined to be faking illness, or malingering, a rule that advocates for the prisoners say discourages them from making or pressing their medical complaints.
“Surgeries are delayed, diagnoses are delayed, until it’s too late to do anything,” Melvin Thornton, an inmate who led a petition drive seeking wider coronavirus testing, wrote in an email. “They can’t deal with that, and then you add a pandemic.”
Angola takes its name from a plantation that once occupied the land on which it was set, in a deep bend of the Mississippi River. Most prisoners now work those same fields, picking soybeans and okra for as little as 4 cents an hour.
For years, Angola was notorious for its violence, a place where guards brutalized the inmates and inmates beat, raped and murdered one another as a matter of routine. Nowadays, it is better known as a monument to mass incarceration, filled with aging, often medically fragile inmates. Three-fourths of them are African American. Virtually all were sentenced to hard labor; most serving life without the possibility of parole.
The medical treatment of Angola’s prisoners has been challenged in the federal courts almost continuously since 1971. Deficient health care — along with rampant violence, overcrowding and racial segregation — led to a federal consent decree in 1983 and supervision by a federal judge of reforms across the state corrections system.
Angola was especially slow to comply; it remained under federal oversight for the next 16 years.
As the violence diminished, state officials drew attention to improvements like the prison law library, educational programs and an elaborate system of privileges and rewards for inmates who followed the rules. But the health care problems proved more intractable.
“Prisoners report horror story after horror story,” lawyers for the plaintiffs wrote in their 2015 complaint. “A man denied medical attention four times during a stroke, leaving him blind and paralyzed; a man denied access to a specialist for four years while his throat cancer advanced; a blind man denied even a cane for 16 years.”
A team of leading prison-health experts, hired by the lawyers to evaluate Angola’s health system, called it “one of the worst we have ever reviewed.” For years, Louisiana prisons have consistently recorded the country’s highest mortality rate. With proper care, the experts concluded, many of those inmates might have survived. “It is our opinion that these preventable excess deaths are a consequence of the systemic inadequacies in the health program,” they wrote.
When the pandemic struck, some of the same civil rights lawyers sued to block a state plan to quarantine coronavirus patients from parish jails in an abandoned punishment block at Angola known as Camp J. But Dick upheld the plan, saying the advocates’ claims that dozens or even hundreds of prisoners could die were “based primarily on speculation and conjecture.”

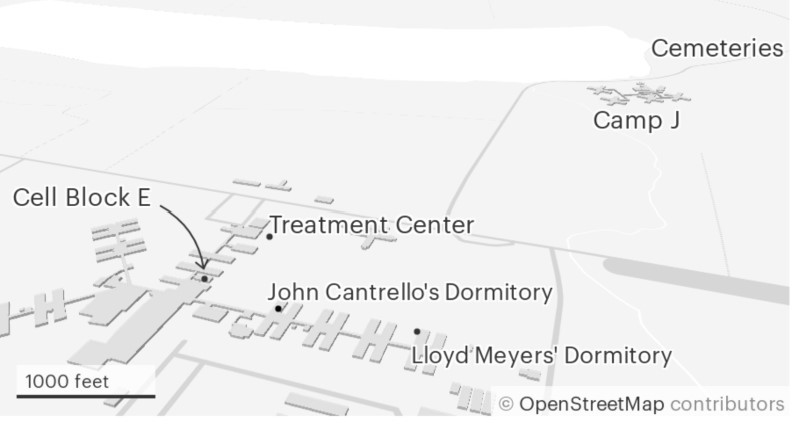
Angola’s Camp J, a once-notorious punishment block that was closed in 2018, has been used in recent months to quarantine inmates who have become infected with the novel coronavirus.
State records show that in mid-February, more than three weeks before Louisiana registered its first COVID-19 case, Morrison began contacting state health officials about the pandemic threat. He also directed prison wardens and doctors to review existing manuals for outbreaks of infectious disease.
By March 12, three days after Louisiana’s first documented coronavirus case, the state’s prisons suspended family visits, tours and other outside contacts. Officials also began “reverse-quarantining,” isolating medically vulnerable inmates at Angola and elsewhere from people who might infect them. “We are taking any measures we can in an attempt to keep the virus from entering our state-run facilities,” Morrison wrote in an email that day.
In a recent interview, Morrison said he believed from the start that extensive testing for the virus would be an essential component of the corrections department’s response. Although Louisiana faced the same shortage of test kits in March that constrained other state governments, Morrison pushed to obtain the largest possible supply of test kits and contracted with a private laboratory to help.
But in mid-April, before substantial testing had even begun, Morrison left the corrections department to return to the LSU faculty, a change he said he had been planning for some time. When he left, he said: “We had plenty of tests available to us. We were telling them to test people. They were sending tests out to the prisons as needed. We told the facilities, let us know when you’re low.”
Early outbreaks erupted at two women’s prisons in the state system. When the authorities tested about 500 inmates in those facilities, they found infection rates of 87% in one and over 60% in the other, Pastorick, the corrections spokesman, confirmed. Those relatively small prisons remain the only ones where mass testing has been done.
The wardens at Angola did not follow suit, even though inmates said many were falling ill and a guard lieutenant had died from the virus in late March. The corrections department has been more willing to test guards and other staff who work inside the prisons, reporting more than 1,000 tests by June 22, with about 19% of them positive.
Corrections officials said that the medical staff at Angola worked to educate inmates about the virus, warn them of the risks and prepare them to protect themselves. But many prisoners said they were told nothing about how to prevent the spread of COVID-19.
Darrill Henry, who was in his 16th year of a life sentence for double murder, noticed that “free folks” — as inmates call the guards and medical staff — suddenly began wearing face masks. One guard vomited in a hallway; others began missing work. “I’m wondering what’s going on,” he recalled. “Nobody is telling us anything. Then, we see on TV, they’re talking about coronavirus every day.”
When the prison staff finally began to distribute cloth-and-string masks weeks later, most inmates wore them for about a week, Henry said. Then many of them stopped, seeing the protection as insufficient, meaningless or just bothersome.
Other efforts at social distancing were minimal at best, inmates said. As late as early April, prisoners were still being taken out into the fields to work in crews of as many as 160. When inmates became concerned about their close quarters, guards suggested they bunk “head to foot” to avoid contact.
Before Henry was released in May — his conviction was overturned and a judge ordered a new trial after exculpatory DNA evidence emerged — his dormitory had been under quarantine almost continuously since the pandemic hit. Even so, he said, some obviously sick inmates were left in their bunks for days. Others were removed to treatment areas or designated isolation quarters only to return, after more contact with sick inmates, a few days later.
Morrison, in consultation with the Centers for Disease Control and Prevention, instructed doctors to look out for fever, cough and difficulty breathing. But at Angola, doctors and nurses generally saw only a small fraction of patients who made it past their screening teams. And the screeners, a combination of guard-paramedics and untrained staff (including assistants from the dental office), appeared to interpret the criteria differently, many inmates said.
As Morrison was leaving the department, one Angola prisoner, John Cantrello, 69, began to have trouble breathing. Cap, as he was known, an obese man who used a wheelchair, called for help four or five times, men in his dormitory said. Each time, his temperature was below the 100-degree threshold that Morrison had set. (The CDC recommended 100.4.) Cantrello was left in his bunk.
“He looked like he was hyperventilating on the phone trying to call his people on the street,” recalled Haller Jackson, who lived in the same dorm. “He was flailing. It was like watching a drowning man.”
Cantrello was finally taken by ambulance to Our Lady of the Lake Hospital in Baton Rouge, where he tested positive for COVID-19. He died three days later, on April 18 — the first inmate death reported by the corrections department.
In another dormitory not far away, a second 69-year-old man, Lloyd Meyers, was having similar troubles. Meyers, an inmate minister, had difficulty breathing, wasn’t eating and couldn’t get out of bed. But he, too, failed to register a temperature high enough to get seen by a doctor.
“He was sick as a dog,” said Michael Zihlavsky, who lived in the same dormitory. “He tried to get help two or three times through sick call, but they wouldn’t do anything for him. They said, ‘Call us back if you have a fever.’”
Finally, Meyers was taken by ambulance to the Baton Rouge hospital, where he, too, tested positive for COVID-19. He died there a day after Cantrello.
Late on the morning of April 25, after President Donald Trump suggested in a White House news conference that sunlight might kill the novel coronavirus, Jackson watched in disbelief as guards ordered the occupants of his dormitory to haul their mattresses and pillows out to a prison yard to be purified. The men left their beds on a basketball court for about an hour, while a team of inmates scoured the dormitory with undiluted bleach.
By then, Jackson estimated, most of the 86 men in his dorm were already infected. Ten of them had been taken to a makeshift coronavirus isolation ward in a shuttered part of the prison. Jackson estimated that an additional 30 men had symptoms of the virus — cough, aches, fatigue, shortness of breath — but they were never tested.
Jackson was sick, too, as he had anticipated. A former lawyer who was caught in a sting operation after arranging online to pay for sex with a person he thought was a 10-year-old boy, Jackson had completed the coursework for a doctorate in epidemiology at Tulane University. (Several years before his arrest, he graduated from Tulane’s law school with the highest grade-point average in its history.)
In Jackson’s dormitory, as in others, men shared just a handful of showers and toilets. When the prison allowed them to contact their families with two free telephone calls a week during the pandemic, many breathed into the same few phones.
Jackson did not expect hospital-grade hygiene. Still, he was shocked by the prison’s difficulty with even basic containment measures, and he was even more dismayed to see how the medical staff cared for those who got sick.
One morning, as infections in his dorm seemed to be peaking, Jackson awoke to find guard-paramedics checking on a man who had collapsed and was struggling to breathe. He had been showing symptoms of the virus for more than a week but was diagnosed with dehydration.
Another man called the EMTs to complain of chest pains; he was diagnosed with gas. “Two guys with terrible migraines vomited and passed out, which could be cardiac symptoms,” Jackson recalled. Although they were taken away by ambulance, the two men were brought back to their dormitories the same day.
In addition to regular “sick calls” by paramedics, coronavirus screening teams moved through the prison daily, pointing their infrared thermometers at the forehead of each inmate to take their temperature. But several prisoners reported getting readings so low — sometimes 93 and 94 degrees — that they should perhaps have been treated for hypothermia.
Studies have shown that such devices can be less accurate than other types of thermometers. But the more serious problem may have been that fever of over 100 degrees was used as the one overriding criterion to determine whether a sick inmate required medical attention.
Although fever has always been the benchmark symptom of infection, the CDC’s clinical guidance on Feb. 12 cautioned that “the fever course among patients with COVID-19 is not fully understood; it may be prolonged and intermittent.” In April, a study of 5,700 patients hospitalized in New York showed that fewer than one-third had fevers when they were admitted. (Other studies have shown considerably higher percentages.)
One Angola inmate, who spoke on the condition he not be named, said that during a two-week period in which he had been most sick — he had trouble breathing, body aches and a loss of appetite, among other symptoms — the screeners told him repeatedly that he did not meet their criteria for assistance.
“You ain’t got no fever, so there ain’t nothing we can do for you,” the man quoted them as saying.
Medical screening at Angola has long been a contentious issue. Under normal circumstances, inmates are required to pay for medical attention, and they ask for it only sparingly. A routine “sick call,” as it is known, costs $3 — a huge sum that low-level workers might labor 75 hours to earn. Emergency calls cost $6, and even paying that amount does not guarantee that an inmate will be seen by a nurse or doctor. Those fees have been temporarily waived during the pandemic.
The experts also highlighted the mistrust of the Angola medical staff — from the medics and nurses to physicians — as a fundamental problem with the system of care.
The paramedics who normally screen patients seeking medical care vary widely in their training; some have as few as 140 hours. Still, they regularly dispense medical care and even medicine without being licensed to do so, according to an expert who testified in 2017 in the federal lawsuit. And while doctors and nurses are supposed to supervise the paramedics closely, they rarely do, the expert said.
The result is that the EMTs make daily judgments about which inmates are truly sick and which might be faking in order to escape work or some other circumstance. They often do so without meaningful examinations, medical records or even medical equipment, much less laboratory tests. “Thus,” the experts wrote in court filings, “it is not surprising that virtually all EMT assessments are inadequate.”
Angola’s medical chief, Lavespere, said in a court deposition that he shares the skepticism with which paramedics often view inmate medical complaints. “The biggest challenge providing medical care at Angola is who is telling the truth,” he said. “People don’t want to go to work. So, you know, a lot of them use the medical department for reasons not to go to work.”
Lavespere’s views may have been shaped by his own experience behind bars: He served two years of his three-year federal sentence for buying methamphetamine with the intent to distribute it. (According to the state medical board, he was also diagnosed with amphetamine, cocaine and marijuana addiction, along with a psychological adjustment disorder with antisocial, narcissistic and avoidant features.)
Like most Angola doctors, however, Lavespere was permitted to resume his medical practice on a probationary status, while restricted to institutional settings like a prison. He has said he felt “a calling” to serve at Angola. But he appears to have had few other options.
Singh, who preceded Morrison as the corrections department’s medical director, said the state board routinely recommended Angola and other prisons to physicians who had lost their licenses for criminal, ethical and substance-abuse issues. He had struggled to recruit doctors with “clean” licenses, Singh said, because they rarely wanted to work in Angola’s remote, high-stress environment. Using doctors with licensing problems, he said, was the “Louisiana solution.”
Apart from a psychiatrist whom Singh recruited from LSU (and who earned a salary of nearly $322,000 last year, more than double that of the state’s corrections chief), all the staff physicians now at Angola have had licensing issues. Including Lavespere, at least three dispensed drugs illegally, were addicted to illegal drugs or both. One committed sexual misconduct with a patient; another struggled with alcoholism.
(Singh was dismissed in 2018 after a sexual harassment complaint by a colleague who said he drunkenly hit on her during a social event at a Lake Charles casino. He sued the department for defamation, and the case is still pending in a state court.)
Prisoners at Angola did not dispute that some might occasionally feign illness. But lawyers in the federal suit have argued that the medical staff’s mistrust defines a system in which truly sick inmates are often examined inadequately or even have their problems ignored. Since the pandemic, the prisoners said, the shortcomings of that system have only multiplied.
Patrick Johnson, a 46-year-old inmate serving a life sentence for second-degree murder, fell sick on April 4, with chills, sweats and dizziness. When the screeners took his temperature, it was 98.2 degrees. After he persuaded them to try again it registered 100.4 — just high enough to be taken to the prison hospital. But when his COVID-19 test came back negative, he was sent back to his dormitory.
Over the next 10 days, his condition deteriorated. He made five more sick calls but was left in his bunk each time. “I wasn’t sick enough to be seen by a doctor,” he said he was told. Finally, with his temperature over 101 and his blood-oxygen level dangerously low, he was rushed to the hospital, where he overheard a nurse tell a doctor he might not survive the night.
When the hospital tested him again for COVID-19, the result came back positive.
In a court declaration on April 1, less than two weeks before he quit as the corrections department’s medical director, Morrison emphasized that he was consulting closely with the Louisiana Department of Health. But according to current and former state officials, that collaboration did not last.
On April 8, the Health Department’s senior official for emergency preparedness, Dr. Jimmy Guidry, issued a short, seemingly straightforward set of recommendations for the state’s prisons and jails. A similar advisory had already been sent to Orleans Parish, where the jail was facing a serious outbreak.
Hands should be well-washed, the state-level advisory said. Coughs and sneezes should be covered. Sick inmates should be isolated in “sick rooms.”
Only the final bullet point stuck out: Prison officials should try to keep all inmates 6 feet apart, it said. If that was impossible, health officials recommended, corrections officials should work with prosecutors, judges and others “to reduce the size of the jail population of the least non-violent inmates.”
Similar steps were being taken in many other states. Probation officers and parole boards were already recommending steps toward the release of some people jailed for less-serious offenses. Still, the suggestion so angered the corrections leadership, those officials said, that the Health Department was forced to immediately withdraw the advisory.
That same day, April 9, the corrections department issued a long, public litany of steps it had taken to mitigate the spread of the coronavirus. Separately, Edwards announced that the department was compiling a list of state prisoners eligible for medical furloughs. (As of June 1, when the furlough program was discontinued, the state had released only 66 of 594 inmates it considered, according to official figures.)
The two advocacy groups that sued the state government to try to block the transfer of prisoners into Angola from parish jails, the Promise of Justice Initiative and the Southern Poverty Law Center, emphasized the decrepit conditions of Camp J, a notorious cellblock that had been shut down in 2018.
Singh, the corrections department’s former medical director, called it “a dungeon.” In court statements and interviews with ProPublica, inmates described the cells there as coated in black mold, with rusted metal toilets and a large population of spiders.
Dick, the federal judge, was not persuaded, noting that the state had cleaned up the camp and retrofitted it with air conditioning before the jail patients arrived. She also ruled that it was reasonable for state officials to remove those inmates from jails where they could spread the virus and quarantine them at Angola, even if the conditions were less than ideal.
With limited testing, Louisiana has registered about 21 positive inmates per 1,000 — a rate significantly higher than the 5 per 1,000 in the general public. Some states that have conducted mass testing in their prisons have reported much higher rates, including Connecticut with 110 per 1,000, New Jersey with 145 and Tennessee with 121.
Lauren Brinkley-Rubinstein, an assistant professor of social medicine at the University of North Carolina, said she viewed Louisiana’s reported numbers with suspicion. It is one of only two states, she noted, that separately counts inmates who test positive but are deemed “asymptomatic.”
“It seems to be a way to protect themselves, to say, ‘Hey, look, everybody here is asymptomatic so we don’t have to worry about anything — there is no serious COVID here,’” said Brinkley-Rubinstein, who is also an investigator with the COVID Prison Project, which tracks the pandemic’s spread in U.S. correctional facilities.
Jackson, the Angola inmate who did graduate studies in epidemiology, said he estimated that three-fourths of the 86 prisoners in his dormitory might have been infected. After his release in early June, he took an antibody test. It came back positive.
“My impression is that everybody’s attitude was: ‘We’re definitely not going to test because the results would be horrible, and we’d have to shut the entire place down and we don’t want to do that. Let it burn through here for 90 days and we’ll figure it out.’”
On May 6, two 78-year-old inmates died from complications from COVID-19. Three days later, another two men died and anxiety inside the walls ratcheted up, prisoners recalled. Some started eating cloves of garlic, which they bought from an inmate food concession. Those who could afford it bought orange juice ($1.54 for a 10-ounce can) and honey ($3.26 a jar).
In one dormitory, inmates encircled a warden and demanded to be tested. “It’s not going to happen,” one prisoner said he told them.
In all there were 13 deaths at the prison in May, a figure more than three times higher than during the same month a year earlier. Nine were attributed to COVID-19.
The proportionally low number of coronavirus deaths at prisons around the country, especially when set against the scope of some of the outbreaks, is emerging as a new mystery of the pandemic. California, for instance, has tested about one-fourth of the roughly 115,000 inmates in its state prisons, finding 3,730 COVID-19 cases. But it has recorded only 19 prisoner deaths.
If the true spread of the disease inside Angola has been as wide as many inmates suspect, the prison may have been fortunate to escape with 12 confirmed deaths so far — all but three of the total for Louisiana’s state prisons.
“Louisiana was a state that was hit really hard,” said Morrison, the corrections department’s former medical chief. “Just looking at the numbers should reflect that we were really lucky or we were doing something right.”
But to the inmates who have been building the coffins and laying them in the ground at the prison graveyard, it has been an especially busy time. “These last few weeks we’ve been using a backhoe,” one inmate said.
How many deaths might have been avoided by wider testing or more attentive care is impossible to know. But relatives of Michael Williams said they could not help but wonder.

Rogers prays by Williams’ body as his son, Kevin Cooks, stands at her side at a funeral home in New Orleans on May 15, 2020. (Kathleen Flynn/ProPublica)
Billeaud was Williams’ third defense attorney since he was sent to prison 45 years earlier, but the first to push his innocence claim. Among the facts she focused on were that another convicted armed robber had confessed to the murder, and that the state’s chief witness had changed his account repeatedly. The lead detective in the original investigation also provided Billeaud with an affidavit saying he believes Williams was wrongly convicted.
In late April, Williams told one of his sisters, Terry Rogers, that several men in his dormitory were sick and someone in an adjacent dormitory had died. “This stuff is getting close,” he said. He was likely infected already.
They spoke on the phone every Sunday night, and on May 3, Williams sounded strange. The next night, another inmate called her to say that Williams was sick with a fever and chills. She began making a flurry of calls to the prison the following morning.
“Every number that I called, a different person told me different things.” Eventually, Rogers said, she spoke to a senior guard officer, Robert Wright, who told her he did not have the virus. “He said, ‘I can assure you of that.’”
Williams told relatives he was isolated in a cell behind heavy metal doors. Later, after he was moved, a nurse said he was being given oxygen, fluids and antibiotics but was still having trouble breathing.
Over the next few days, although the family called the prison repeatedly, it got little information. One nurse said he was getting better. But the next day, May 9, a doctor called from Our Lady of the Lake to say that “he wasn’t going to make it.” By the time they arrived, Williams was brain dead.
“He was locked up for 40 years,” Rogers said. “He lived in total hell, and even at the end of his time, they treated him unfairly. Not everyone going to prison is a criminal. And even if they are, if anyone does wrong, it don’t give you the right to mistreat. They still need to be treated when they are sick.”
Claire Perlman contributed reporting.







© 2024 Tucson Weekly
